David Black, Rocío Lopez-Velasco, Horst Hahn, Javier Pascau, Ron Kikinis. Computer Assisted Radiology and Surgery, June 2017
In image-guided interventions, screens display information to help the clinician complete a task, such as placing an instrument or avoiding certain structures. Often, clinicians wish to access this information without having to switch views between the operating situs and the navigation screen. To reduce view switches and help clinicians concentrate on the situs, so-called auditory display has been gaining attention as a means of delivering information to clinicians in image-guided interventions. Auditory display has been implemented in image-guided interventions to relay position information from navigation systems to locate target paths in liver resection marking, resect volumes with neuronavigation, and avoid risk structures in cochleostomy. Previous attempts provide primarily simple, non-directional warning signals and still require the use of a navigation screen. Clinical participants in previous attempts requested auditory display that provides directional cues. Our described method allows screen-free navigation of a tracked instrument with auditory display. However, because changes of y-axis instrument movement onto beneficial auditory display parameters has proven to be difficult in previous work, this paper compares two methods of mapping elevation changes onto auditory position parameter – one using pitch comparison between alternating tones, and another with slightly falling and rising frequencies (glissando) for each tone. In this work, we present a pilot study that compares time-to-target as a performance factor to compare these two methods.
The two auditory display methods are used to relay the position of a tracked instrument using sound. The methods described here relay elevation (changes in the y-axis), azimuth (changes in the x-axis) and distance along the perpendicular trajectory path (z-axis) from the tracked instrument towards a target. Because the methods are suited for applications involving 2D placement plus a 1D depth component, these generalized auditory displays allow tracking during a variety of clinical applications using tracked instruments, including resection path marking, ablation and biopsy needle placement, bone drilling, and endoscopic instrument placement.
Two methods were developed for comparison to relay the position of a tracked instrument using auditory display. Both employ the same mapping for changes in azimuth (x-axis) and depth (z-axis). For changes in elevation (y-axis), the first method employs pitch comparison. A tone with moving pitch between 261 Hz and 1046 Hz is alternated with a reference tone with static pitch of 523 Hz. This alternation allows the user to compare both pitches, bringing one towards another, similar to tuning a guitar or violin string. When the pitch of the moving tone reaches that of the reference tone, the correct elevation is reached. For the glissando (lit. “sliding”) method, only one moving tone is used. When the elevation is positive, the pitches of the tones “slide” down slightly, signaling that the instrument should be lowered. When elevation is negative, the tones “slide” up slightly, signaling that the instrument should be raised. A similar range is used, and the pitch of the tones “slide” ± 3 semitones (ca. ±19%).
For both methods, changes in azimuth are mapped to changes in stereo mapping. The tones described above are played in stereo to indicate whether the target is left or right of the current position. A “sound object” metaphor is employed, for example, when the instrument is to the right of the target, tones are heard in the left ear, indicating that the target is to the left of the listener. Changes in perpendicular distance to the target (z-axis) are mapped linearly to the inter-onset interval (duty cycle) of the tones, similar to an electronic car parking aid. At maximum distance, tones are played 900 ms apart; at the target, this is reduced to 200 ms.
A pilot study was performed with 10 non-expert participants to gauge the usability of each of the methods for elevation mapping. After a short training period with eyes open using a screen to become familiarized with the system, each participant completed two placements of the tracked instrument with eyes closed, i.e., blind placement without screen, for each of the two methods.
For the pitch comparison method, time-to-target averaged 57.1 seconds across all participants. For the glissando method, the time-to-target averaged 23.6 seconds. On a subjective difficulty scale of “low,” “medium,” “high,” and “very high,” half of the participants rated the difficulty of the pitch-comparison method as “low” and half as either “medium,” “high,” or “very high” difficulty. In contrast, all participants rated the glissando method as “low” difficulty. Participants commented on the high mental demand of hearing the reference tone and the task of comparing the two alternating tones.
Although the use of auditory display for image-guided navigation tasks has increased in recent years, previous attempts have primarily provided only basic warning signals, prompting clinicians request directional cues in auditory display. Whereas changes in azimuth can be mapped intuitively to changes in stereo mapping and distance to target can be mapped to inter-onset-interval thanks to participant familiarity with car parking aids, changes in elevation have proved troublesome to design. This pilot study compares two methods for mapping elevation – alternating pitch between two tones (“instrument tuning” metaphor) and sliding pitches for single tones (“glissando”). Results of the study show that the glissando method is promising, leading to reach the target faster and giving lower subjective difficulty rates by participants. Further studies should incorporate additional, refined auditory display methods and evaluate use in real clinical scenarios.

 During medical needle placement using image-guided navigation systems, theclinician must concentrate on a screen. To reduce the clinician’s visual reliance on the screen, this work proposes an auditory feedback method as a stand-alone method or to support visual feedback for placing the navigated medical instrument, in this case a needle.
During medical needle placement using image-guided navigation systems, theclinician must concentrate on a screen. To reduce the clinician’s visual reliance on the screen, this work proposes an auditory feedback method as a stand-alone method or to support visual feedback for placing the navigated medical instrument, in this case a needle.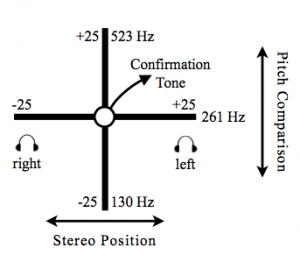 An auditory synthesis model using pitch comparison and stereo panning parameter mapping was developed to augment or replace visual feedback for navigated needle placement. In contrast to existing approaches which augment but still require a visual display, this method allows view-free needle placement.
An auditory synthesis model using pitch comparison and stereo panning parameter mapping was developed to augment or replace visual feedback for navigated needle placement. In contrast to existing approaches which augment but still require a visual display, this method allows view-free needle placement.